

Eyes and Brains
Sometimes I choose my blog subjects based off of a subject that I’m going to be teaching, or other times something I just have a peaked interest in at the moment. Pupils are something I have been meaning to dive into much deeper, and this blog is my first descent. Some might consider this type of physical exam knowledge low yield, but I consider it the coolest thing ever. Pupillary response and cranial nerves are incredibly interesting. Today we will mostly by talking about CN III. Our third cranial nerve, the oculomotor nerve, has several functions that can be easily observed. We will talk about two pathologies that can alter its action today. The first is uncal herniation, the second is brain aneurysm. Here is a quick terminology refresher when talking about pupils:
Anisocoria
Anisocoria means unequal pupils. This could be normal for a patient, or it could be indicative of an acute pathology.
Miosis
Miosis is constriction of the pupil(s). Constriction of the pupils is a parasympathetic response.
Mydriasis
Mydriasis, on the other hand, means pupillary dilation. I always remember the different between miosis and mydriasis by remembering that the larger word means larger pupils. Dilation of the pupils is an action of the sympathetic nervous system.
Ptosis
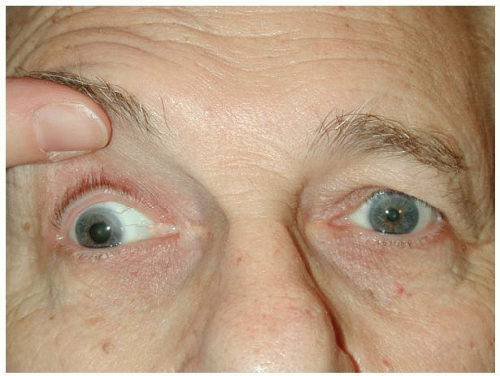
Ptosis is drooping of the eyelid
Down and Out Syndrome
Down and out syndrome refers to CN III palsy. The third cranial nerve has the ability to pull the eyelid open, constrict the pupil, and aim the eye superiorly and medially. Now, imagine the opposite of everything I just mentioned. Unilaterally, a droopy eyelid, a dilated pupil, and an eye that is pointed inferiorly and laterally. This directional aiming is due to now unopposed CN IV and VI stimulation of the eye. What does down and out syndrome mean for us?
Uncal Herniation
Uncal herniation is usually the result of an subdural or epidural hematoma. I remember when I was in school we were taught that when the brain herniates from increased ICP, the brain starts to herniate down the foramen magnum. I believed this for years until I found out that was nearly impossible. Since this space is occupied by the spinal cord (which is apparently not very compressible) it would be very difficult for the brain to herniate through this opening. Instead, what usually happens is uncal herniation. The tentorium cerebelli is what separated the cerebrum (upper brain) from the cerebellum (lower brain). When we get an epidural or subdural hematoma in the upper brain (supratentorial), the next place the brain wants to displace is through the tentorial incisura to the lower brain area (infratentorial). In the process of doing this, it compresses CN III due to the location of this nerve. This causes the down and out syndrome that I explained above (obviously along with other huge problems). It is interesting to note that the side of the down and out eye is the same side as the brain injury/hematoma (ipsilateral).
Be aware that CN III palsy in uncal herniation is an ominous sign to watch out for.

Brain Aneurysms
Subarachnoid hemorrhages usually start with an aneurysm. There are actually two (technically three) types of these aneurysms:
Saccular or “Berry”
Berry aneurysms are the first type, and are named after how the look. They appear as a berry (like the food) sticking off of an artery. There are the most common type of aneurysms that precede subarachnoid hemorrhage.
Fusiform
The second is Fusiform. Fusiform looks like a widening of the entire artery. There is also a second subset in fusiform that includes dissecting aneurysms (third type), which have an outward appearance of a fusiform, but are a little different on the inside.
When one of these aneurysms form, they have the ability to expand and place direct pressure onto the CN III (resulting in CN III palsy). The site that of expansion that would cause CN III palsy would the posterior communicating artery (and sometimes the posterior cerebral artery, internal carotid artery and basilar artery). This artery runs right next to CN III, so any aneurism here has the ability of compressing and inhibiting CN III. Why is this important to know?
There are many things that can cause CN III palsy, I have only included what I consider to be high yield information in this blog. There is so much more to know! Expansion precedes rupture. Sudden onset ‘down and out’ of a unilateral eye is an important sign to pick up on. Also, if you have CN III palsy, but then the palsy suddenly resolves, this could be a sign that a subarachnoid hemorrhage has just occured - blood in the space (subarachnoid) of the previous aneurysm may also cause compression and CN III palsy. Surely, getting this patient to a facility with extensive neurological examination and interventional capabilities would be first priority.
References and Picture Credits
https://www.slideshare.net/fernferretie/brain-herniation-imaging
https://myneurosurg.com/cranial-anatomy/cranial-nerve-3-oculomotor-nerve/
https://entokey.com/ocular-misalignment-and-other-ocular-motor-disorders/
https://www.ncbi.nlm.nih.gov/pubmed/15004590
https://www.ncbi.nlm.nih.gov/pubmed/15337148
https://www.ncbi.nlm.nih.gov/pubmed/11706136